
Roanne K. Jalopy explains the history and haphazard ideology behind medical neglect of the trans community.
People of trans experience are incredibly vulnerable. They are widely discriminated against at school, at work, and are denied access to basic healthcare. But 2020 has been a particularly bad year due to the efforts of conservatives and so-called radical feminists to mainstream discrimination against women of trans experience, and to delegitimize men of trans experience. The common thread of the conservative and so-called radical feminist argument is that anyone who was assigned male at birth is potentially dangerous, and should not be given access to safe spaces such as rape crisis centers and women’s bathrooms.
This fear-mongering is particularly prevalent in the United Kingdom, where even left-leaning newspapers have given it a platform. Guardian columnist Suzanne Moore—who recently resigned after colleagues expressed concern over transphobic content in their paper—complains that “transgender ideology” is a slippery slope that will ultimately lead to women’s legal rights being revoked:
In some transgender ideology, we are told the opposite [of standard feminist belief]: gender is material and therefore can be possessed by whoever claims it, and it is sex as a category that is a social construction. Thus, sex-based rights, protected in law, can be done away with.
There is no effort by trans advocacy groups to do away with sex or body-based rights; the claim that people of trans experience mean to do so is conspiratorial thinking at best. Some radical feminists, aware that their anti-trans stance may look like the typical scapegoating of a vulnerable minority, instead frame their claims in compassionate terms. Children’s author J.K. Rowling gained notoriety in 2019 by coming out in support for Maya Forstater, a tax consultant who lost her position at a think tank after she publicly stated that a proposed law would put women’s rights in jeopardy by allowing “males” into women’s changing rooms. Since then, Rowling has attempted to stir up a moral panic, arguing that gay children are being pressured to take hormone treatment:
Many health professionals are concerned that young people struggling with their mental health are being shunted towards hormones and surgery when this may not be in their best interests… Many, myself included, believe we are watching a new kind of conversion therapy for young gay people, who are being set on a lifelong path of medicalization that may result in the loss of their fertility and/or full sexual function.
To the uninformed reader, it does sound like there’s a crisis. It would be outrageous if people who are happy with their gender were being forced to take hormones and pressured into life changing surgery. But is this really true? And what should we make of Rowling’s puzzling assertion that children of trans experience are actually gay?
In this article, I will attempt to answer these questions and address arguments against fundamental rights from both radical feminists and conservatives. I will draw upon my own experience of transitioning from male to female as a teenager in the early 2000s, as well as the experience of friends who have transitioned more recently. In doing so, I hope to convince the reader that despite Rowling’s alarmist framing, gender clinics have more often than not been a paternalistic obstruction to individuals of trans experience.
Transitioning then and now
To me, the early 2000s seemed like a good time for people of trans experience. A generation of men and women had already shown that it was possible to socially transition and be successful. There were numerous online resources and forums. The country where I lived—the United Kingdom—had a gender clinic especially for children, and in 2004, passed a law allowing individuals to legally change their gender.
I had long questioned the arbitrary nature of the gender binary, and by the time I was in high school I felt confident enough to start cross-dressing. I’d show up to class wearing a skirt, much to the alarm of my teachers (and a few of the other students). Soon, my whole wardrobe was made up of clothes tailored for women. I grew my hair out, and no longer “passed” as male in public. Like many women in my position, I was very insecure, and at first I didn’t realize the extent to which people were reading me as female. The penny finally dropped when I tried to board a flight, and the border guards asked me why I had a boy’s passport.
Up to that point, everything had been so easy. But my school wasn’t at all happy about the changes it had noticed in me: I narrowly escaped expulsion, but only after pledging to stop transitioning until I had graduated. And soon I learned how difficult it was to get an appointment at the Tavistock gender clinic in London, and that it was largely run by men who had their own views on who should be allowed to socially transition.
Access to Healthcare
The United Kingdom is fortunate to have universal healthcare, although decades of privatization and budget cuts mean that it seldom lives up to its name. The way the National Health Service (NHS) is structured means that each region has to fund its own healthcare; this is fine if you live in London, but what if you live in an impoverished part of the country? In practice, many people go without medical treatment, as local authorities are reluctant to use their limited budget to send patients to hospitals outside their catchment area.
As a teenager, I lived in a rural part of the country that had been devastated by the free market policies of the 1980s and 1990s. When I asked my doctor for a referral to the Tavistock clinic in 2004, I was refused outright. There was no point, she explained. We had psychiatrists at the local hospital, and there was no way the local health authorities would pay to send me to London.
After much pestering, and a lengthy appeals process, I did get to see a psychiatrist, but only at the local hospital. And the doctor I saw had never worked with people who were questioning their gender—the patients she usually saw were gay men trapped in a heterosexual marriage. I saw her once, and as she couldn’t send me London and was unwilling to prescribe hormones, there was no point in going back.
But I soon learned that even if my doctor had been willing to refer me to the Tavistock, it would still have been an utter waste of time. The clinic had a waiting list two years long, so by the time I got an appointment I would have been too old, and they would have just referred me to the clinic for adults at Charing Cross, itself with a year-long waiting list.
It was becoming abundantly clear that the only way I was going to be able to access hormone treatment and surgery was if I somehow paid for it myself.
Gatekeeping
I eventually managed to get a private appointment at the Charing Cross clinic, where I saw the late Dr. Richard Green. I didn’t know it at the time, but Dr. Green had been an early LGBT ally. In the 1960s, he had appeared in court to advocate for individuals being discriminated against for their sexual orientation and gender identity. In the 1970s, he had orchestrated a successful campaign to remove homosexuality from the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM).
But the man I saw at Charing Cross was no ally, and the appointment was far from a psychiatric assessment. Dr. Green told me to wait a few years so that I could make up my mind, and that most likely I would end up as a gay man. This was utterly perplexing: I had never been attracted to men, and I’d already spent a great deal of time thinking about my gender. How could Dr. Green think he knew better than me, based on a superficial 30 minute conversation? And why was I paying hundred of pounds for useless advice?
It’s worth taking some time to understand Dr. Green’s position, as he was extremely influential in both North America and the United Kingdom. His philosophy is neatly summed up in this quote from a 2017 paper:
I am convinced that it is a helluva lot easier negotiating life as a gay man or lesbian woman than as a transwoman or transman.
This is a puzzling assertion: why would a girl of trans experience grow up to be a gay man? How could an “expert” who has studied gender his whole life conflate gender identity with sexuality?
Green’s belief stemmed from a study he carried out in California through the 1980s, in which he psychologically examined a cohort of 66 externally assigned boys whom he considered “feminine.” Of the 44 individuals Green re-examined as adults, 18 were primarily attracted to men, 14 were attracted to men and women, and 12 were primarily attracted to women. One individual continued to identify as a woman into adulthood.
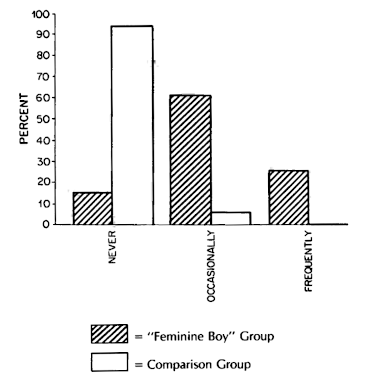
In a remarkable leap of logic, Green concluded that the children grew up to be attracted to men instead of identifying as women, as if the two outcomes were mutually exclusive. But very little can be concluded from this study. For a start, only 30 percent of the children frequently said they were girls, so it’s unsurprising that so few identified as women in adulthood. What’s more, there was no realistic pathway for the children to socially transition in the 1980s. Green himself called them “sissy boys,” refused to acknowledge their gender identity however stated, and actively worked with parents to make them conform. He describes his “treatment” of one child (note that he misgenders the child throughout):
My goal with his parents was to discourage any support of his cross-gender behaviors, and to encourage boyish behaviors that were compatible for father and son… During an early session with the boy, the irrevocability of being a boy or a girl was stressed.
So Green effectively prejudiced his own study.
Although a lot more research has been carried out since the 1980s, much of it is unreliable. Kenneth Zucker, a Toronto psychiatrist who has published a formidable number of studies on gender identity, had the same approach as Richard Green. He would instruct parents to take away toys he deemed inappropriate to the child’s externally assigned gender, and considered it his goal to “reduce [the] child’s desire to be of the other gender.”
A slightly better body of evidence has come from the V.U. University Medical Center in Amsterdam. Although the center still considers trans experience to be a diagnosable mental illness (in the past “gender identity disorder,” now gender dysphoria), it does treat adolescents with puberty blockers. In a 2013 paper, the center reported that out of 127 individuals they had assessed as children, 47 returned as adolescents (over age 12) and were prescribed puberty blockers. Unsurprisingly, the children who had persistently said that their gender differed from that assigned at birth were far more likely to return for medical treatment.
The V.U.’s approach is clearly better than Green’s, although I question the value of sending under 12s to a gender clinic. These clinics tend to base their practice in psychiatry or psychoanalysis, two fields that have a long history of gender essentialism and can offer little to children who are questioning their gender. Children do need support, but it needs to come in a form that treats the child as an individual and not a medical subject. Most doctors have never seriously questioned their gender, and are poorly equipped to help a child figure out her own relationship to gender. Too often, these “specialists” have their own preconceptions, and even if well intentioned, try to shepherd their patients towards stereotypical behaviors. Under these circumstances, children are quick to realize that their only way to be taken seriously is to jump through the clinician’s diagnostic hoops.
This is exactly what I faced under Richard Green at Charing Cross: he made it clear that he wouldn’t prescribe anything (even testosterone blockers) until I had socially transitioned. And I knew from other women I’d met online that the only way Dr. Green would have taken me seriously is if I had transformed myself into a caricature of femininity—and I say caricature because I would have been pretending to be someone I’m not. I had no interest in transitioning in order to conform to someone else’s standard of what it is to be a woman.
Malpractice Investigations
I was totally discouraged by my experience at Charing Cross. I realized I was facing years of fruitless “psychological assessments,” whose real aim was to force me to accept the gender I had been assigned at birth. The most cruel and unusual practice was the so-called “real life test.” Rather than providing as much support as possible for an incredibly difficult step, the psychiatrists withheld hormone treatment until their patients had socially transitioned for at least three months. Even after this period, they could still refuse treatment if the individual did not live up to their preconceived idea of gender. For adults, this meant attempting to transition without the physical changes brought on by hormone therapy. In my case, it meant going further through a puberty I didn’t want.
I didn’t have years to wait. My body was starting to change in ways I didn’t like, and if things continued, I’d have to pay hundreds of pounds that I didn’t have on painful facial hair removal, and figure out how to un-drop my voice. Like many women, I chose to self-medicate with testosterone blockers and estradiol pills ordered from an overseas pharmacy. This was both expensive and risky—there was no way of knowing if the pills were genuine or not, and the NHS refused to monitor individuals who self-medicated, despite providing regular endocrinological checkups to patients at the gender clinics.
Fortunately, after a year of procuring pills on the black market, I managed to see a doctor who was prepared to help. Dr. Russell Reid ran the Beaumont Trust, the first charity in the United Kingdom dedicated to gender diversity, and didn’t believe in medical gatekeeping. He asked me if I was certain I wanted to transition medically, and suggested I talk things over with a psychotherapist, but was happy to prescribe testosterone blockers on my second visit.
I only saw Dr. Reid twice before he was suspended from practicing medicine. The gender clinics run by the NHS took a dim view towards any doctor who rejected their orthodoxy. Dr. Reid was investigated for malpractice—to the directors of the Charing Cross clinic, his practice of prescribing hormones without a real life test was “collusion between him and the patient.”
More seriously, five of Dr. Reid’s patients regretted their gender affirmation surgery. These cases are incredibly upsetting—one individual, known as Claudia, had already socially transitioned and was pressured into getting surgery by her partner, who wanted to “fix” her. We’re now coming to accept, as a society, that it’s fine to socially transition without seeking surgery, and I hope that sad cases like Claudia’s will be rarer. But it’s also important to have some perspective: these five individuals represent a tiny fraction of Dr. Reid’s patients. And in recent years, two of the women have admitted that they detransitioned because of peer pressure—one had been pressured by her church, the other by her family. This is reflected in the statistics: true regret is rare, and the usual reasons for detransitioning are financial and social pressure.
Since Dr. Reid’s suspension, doctors who have attempted to run their own gender clinic have been similarly investigated after patients have expressed regret. But if we are to stipulate that no one should ever regret transitioning, every gender clinic in the world (even Charing Cross) would have to close. Moreover, this stringent condition for remaining in practice reveals a bias in the British medical establishment: the well-being of innumerable individuals of trans experience is deemed less important than that of the handful who regret transitioning.
Has anything changed?
The medical gatekeepers are slowly disappearing: Richard Green passed away in 2019, and Kenneth Zucker was fired from his Toronto clinic in 2015 over his outdated practice. The Tavistock clinic is now committed to a less paternalistic approach, and more clinics have opened outside London. In the United States, there are numerous clinics that are willing to prescribe gender affirming hormones to adolescents.
In spite of these changes, it’s now more difficult than ever to access treatment. The simple reason is that far more people are seeking referral to the gender clinics. When I was a teenager, perhaps 100 people a year sought treatment in the United Kingdom. Now the number is in the thousands, with waiting lists three years long. In one case, a teenager waited two years for an appointment at the Tavistock clinic, was told he was too old and had to wait 4 years for an appointment at Charing Cross. He committed suicide.
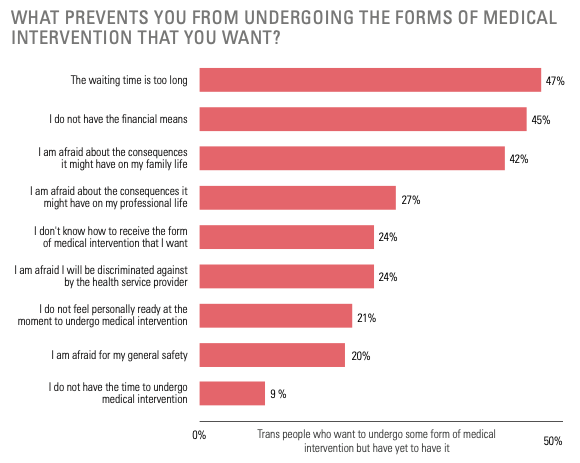
A 2017 report from Stonewall found that even today, a quarter of those who seek medical treatment do not get it. The main reasons? Long waiting times at public clinics (so many people still have to procure hormones from the black market), and no financial means to pay for private treatment. The situation in the United States is similar: the 2015 Transgender Survey found that a quarter of respondents had been denied hormone treatment by their health insurance provider.
Although the management at the gender clinics has changed, the new guard are far from the ideologues that J.K. Rowling imagines. No one is being “shunted towards hormones and surgery.” A younger friend, a woman of trans experience who went to the Tavistock clinic aged 13, tells me that they didn’t take her seriously because she showed up wearing jeans and a T-shirt. Her doctor also brought up the fact that she was an immigrant, and suggested that she might be seeking treatment due to cultural pressures. She was only prescribed testosterone blockers and hormones when she was 18.
We can get a better view of the inner workings of the Tavistock clinic from an action plan it published in 2019. It paints a picture not of ideological uniformity, but an attempt to find a middle road between the “extremes” of the “trans-affirmative” and “trans-critical” lobbies:
A particular issue that emerged for the trust and clinical staff within the service has been the pressure from strongly held views by various pressure groups, namely the trans-affirmative and trans-critical lobbies. This continual interest, critical scrutiny and often very strongly held opinions has created an atmosphere of significant persecution for staff and the need to repeatedly address some of the issues emerging from groups having definite agendas. At the same time, it is worth acknowledging that some of these views and extremes of opinion can be reflected within the staff group.
It’s harmful enough that these psychiatrists are acting as cautious gatekeepers, but what’s even worse is that access to treatment is now in the hands of an even less qualified elite. The High Court of England and Wales has recently made it virtually impossible for under 16s to access puberty blockers: in a throwback to the gender policing of the 1980s, the justices made the perverse argument that the treatment must be banned precisely because most children who start on puberty blockers go on to take hormones. The only way around this ban is to gain express permission from the court, meaning treatment is now restricted to the tiny minority who have the financial resources to mount a legal challenge.
Despite the promising trends in the medical profession, life is still difficult for people of trans experience. Because of the cost, and the lack of willing doctors, medical transition is not universally possible. Psychiatrists, most of whom have again never questioned their own gender, continue to use gender essentialist criteria to decide who is allowed to transition. The recent high court ruling in the United Kingdom will cause untold damage to a whole generation of young people who will have no choice but to undergo an unwanted puberty that can never be fully reversed.
The Societal Backlash
Despite all the roadblocks to transition, people of trans experience are more visible than ever before. This has led to considerable backlash. The main opponents remain conservatives and the so-called radical feminists: both groups make similar arguments, and none of these arguments are new. Like the psychiatrists of yesteryear, they tend to focus almost exclusively on women of trans experience: the radical feminists tend to bring up perceived dangers to other women, while conservatives appeal directly to biological essentialism and focus on the “imposition” of having to use correct pronouns. Both groups are uneasy about the use of puberty blockers and allowing children to socially transition. It’s worth looking at the main arguments these groups use, one by one.
Gender clinics are are practicing “a new kind of conversion for young gay people”
Let’s return to J.K. Rowling’s tweet where she condemned so-called “conversion therapy”:
Many, myself included, believe we are watching a new kind of conversion therapy for young gay people, who are being set on a lifelong path of medicalisation that may result in the loss of their fertility and/or full sexual function.
As discussed earlier, today’s gender clinics do not try to convince children to transition socially or to take hormones, and they are well aware that gender and sexual orientation are two different things. The clinicians with a history of conversion therapy are now gone, and their “therapy” was the opposite of what Rowling imagines: they were trying to convince gender non-conforming children to be gay.
Yet Rowling is nostalgic for this era of gatekeeping:
I happen to know a self-described transsexual woman who’s older than I am and wonderful. Although she’s open about her past as a gay man, I’ve always found it hard to think of her as anything other than a woman, and I believe (and certainly hope) she’s completely happy to have transitioned. Being older, though, she went through a long and rigorous process of evaluation, psychotherapy and staged transformation.
In other words, Rowling isn’t against preventing women from transitioning as such, but her acceptance is conditioned on her own willingness to think of the person as a woman. This is nothing more than gender essentialism, and a peculiar double standard: surely Rowling has no objection to people who were assigned female at birth going against gender norms? And if the issue is that the woman in question went through a “rigorous” and presumably difficult process of transition, why should transitioning be rigorous and difficult in order to make a person of trans experience qualify as a woman in Rowling’s eyes?
“I’m not going to modify basic biology because it threatens your subjective sense of what you are.”
Conservatives tend to be more overt about their gender essentialism. Ben Shapiro refuses to use pronouns that do not match a person’s externally assigned gender, arguing that basic biology says that there are only two sexes. While it is possible to construct such reductionist categories, the way people are “gendered” in society has almost nothing to do with the physical reality of their sexual organs. Does Shapiro insist on inspecting a person’s genitals before deciding which pronouns to use? If not, how can he be sure that he’s using the pronouns that follow his narrow definition?
As with Rowling, Shapiro’s problem is with people he perceives not to conform to his narrow definition of gender; the issue, in short, is his subjective sense of what people are.
“A lot of people change their mind”
J.K. Rowling is also worried that many will regret their gender affirmation surgery:
I’m concerned about the huge explosion in young women wishing to transition and also about the increasing numbers who seem to be detransitioning (returning to their original sex), because they regret taking steps that have, in some cases, altered their bodies irrevocably, and taken away their fertility.
Regret after surgery is a terrible outcome, but as I mentioned earlier it’s nowhere near as widespread as Rowling suggests. Of 3398 individuals seen by the Charing Cross gender clinic between 2016 and 2017, only 16 regretted transitioning. In the United States, the 2015 Transgender Survey found that 8 percent of respondents reported “detransitioning” at some point, but the majority had done so due to peer pressure. Only 0.32 percent of respondents had reverted to their externally assigned gender of their own volition, and we don’t know how many of them had gender affirmation surgery. Like the psychiatric gatekeepers, Rowling values the few who detransition over the thousands whose lives are transformed for the better.
“Autistic children are being misdiagnosed”
Although she has never previously shown concern for neurodiversity, Rowling is deeply troubled that children who have autism are transitioning:
The UK has experienced a 4400 percent increase in girls being referred for transitioning treatment. Autistic girls are hugely overrepresented in their numbers.
She’s not alone. Joe Rogan, a popular podcast host, claims that these children are socially transitioning just so they can get attention:
Large clusters of kids who are mostly kids that are socially awkward, many of them are autistic, many of them have never had any praise at all in their life, and they transition and they get all this praise from people. Because it is, right now it’s in vogue.
There is very little quality research on neurodiversity in people of trans experience—most of it relies on psychometric questionnaires, though the few studies of clinical diagnoses of autism suggest a prevalence of 6 to 26 percent, which is higher than in the general population.
But to be clear: autism does not mean an inability to make decisions about one’s life. There’s no reason to doubt the gender identity of a child of neurodiverse experience more than that of any other child. And the idea that children who have been neglected and bullied are gaining acceptance after socially transitioning is fanciful. The 2015 Transgender Survey’s findings are bleak: 77 percent of school children who were perceived to be “transgender” had been bullied, physically attacked, or expelled.
Puberty blockers are an “unregulated live experiment on children”
Carl Heneghan, who runs the Centre of Evidence-based Medicine in Oxford, has criticized the use of puberty blockers:
Given paucity of evidence, the off-label use of drugs in gender dysphoria treatment largely means an unregulated live experiment on children.
He is referring here to gonadotropin-releasing hormone agonists (GNRHa), which were developed to treat precocious (excessively early) puberty in both boys and girls, and have been in use for almost 40 years. This medicine has been extensively researched:
- Two studies followed a combined total of 137 girls who were treated for precocious puberty. Neither study found any long-term health issues, and following treatment, the girls had no associated health issues in adolescence and early adulthood.
- A long-term study followed nine boys who were treated with GNRHa for an average of five years, to delay their precocious puberty. After stopping treatment, their puberty proceeded without issue. They all had normal endocrine function, and none of them had any problems with bone density or fertility.
GNRHa has been used for over 20 years to suppress puberty in adolescents of trans experience. All the evidence suggests that if these adolescents do change their mind, their puberty will resume after they stop taking the blockers. The current recommendation for endocrinologists treating children of trans experience is to prescribe GNRHa at the first sign of puberty, and testosterone or estrogen at age 16—when the adolescent is old enough to make a decision. Most continue on to hormone treatment: of 70 adolescents who were treated in Amsterdam between 2000 and 2008, none changed their mind.
The alternative is to delay medical treatment until adulthood, which has much worse outcomes. The effects of puberty can only be partially reversed with painful and expensive surgery, and people who were denied puberty blockers are far more likely to consider taking their own life as adults.
So what are Dr. Heneghan’s criteria for evidence? Rather than better studies, it sounds like he’s calling for a total and complete shutdown of the use of puberty blockers. Isn’t that, in its own way, a live experiment on children who do not identify with their assigned gender?
“The transgender suicide rate is 40 percent… It makes virtually no difference, statistically speaking, as to whether people recognize you as a transgender person or not.”
A common talking point, repeated by Ben Shapiro among others, is that social transition makes no difference to the suicide rate. The actual suicide rate is unknown—death certificates don’t record trans experience—although around 40 percent of people of trans experience do report having attempted suicide.
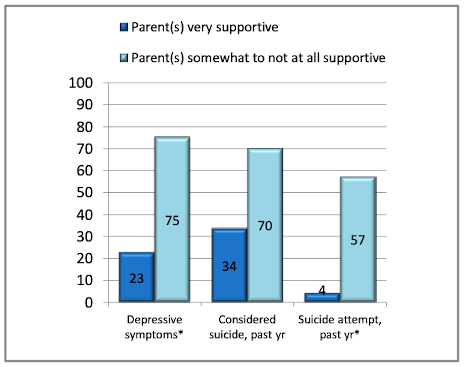
A fair comparison of suicide rates is difficult, as there is limited data on individuals who are not being seen at a gender clinic. But a survey of 433 individuals from Trans PULSE, a community-based research project in Ontario, suggests that people with a supportive family are unlikely to attempt suicide.
This ties in with research which shows that children who are allowed to transition socially have much better mental health than those who are not allowed to transition. When compared to a gender-matched control group, children who had socially transitioned were found to be no more likely to suffer from depression, and had only marginally higher levels of anxiety. We will see how they fare in future, but the initial results are promising.
A related talking point is that gender affirmation surgery is useless, as there is a high suicide rate even after the surgery. The origin of this claim is a study from Sweden that compared individuals who had chosen to have surgery to the general population. This was a very limited study: it gave no indication of the suicide rate before surgery, and did not look at successful social transition, a far more important indicator of wellbeing.
More recent research that looked at everyone in Sweden who had a “gender incongruence diagnosis” found that people were less likely to seek mental health treatment after gender affirmation surgery.
“Allowing trans women access to protected spaces puts women in danger”
In the Economist, so-called feminist Kathleen Stock disagreed with a proposed law that would make it easier for people to update their birth certificate to reflect their gender identity, suggesting that “changing the concept of ‘woman’” will have terrible consequences:
There’s also a separate worry that violent males who do not consider themselves trans will eventually take advantage of increasing confusion about social norms about such spaces. Sex offenders already go to great lengths to access vulnerable females; there’s no reason to think they wouldn’t use this situation to their advantage.
It has already been pointed out that predators can simply walk into female spaces—no one checks birth certificates at the door. And rape crisis centers, which protect some of the most vulnerable women, have been open to women of trans experience for years, without any issues.
But Stock goes on to make a specific statistical claim:
Note that this is emphatically not a worry that self-declared trans women are particularly dangerous or more prone to sexual violence. It’s rather that we have no evidence that self-declared trans women deviate from male statistical norms in relevant ways.
What evidence would Stock admit that would overcome her assumptions? We already know that people of trans experience, far from being perpetrators, are disproportionately victims of violence. Like many others we’ve discussed, Stock places the bar of evidence so high as to be unsurmountable, and provides no indication of what would be required to convince her. The simple word for this is prejudice.
What lies ahead?
It’s hard to cover access to medical care without touching on the fact that the richest country in the world doesn’t have universal healthcare, and market reforms have eroded coverage elsewhere. As the gap between rich and poor increases, hormone treatment and surgery are becoming a privilege for the wealthy few. In my own case, I still don’t really have access to healthcare. I can just about convince a general practitioner to prescribe estrogen patches, but I’ve never had a proper endocrinological assessment, and if something were to go wrong, I have no confidence in the quality of care I would receive.
Although gender clinics are becoming more supportive, they have not universally adopted a gender affirming approach and are, on the whole, still tied to a normative concept of gender. This isn’t just a criticism of gender clinics—these biases are a reflection of society as a whole. Despite the conservative hysteria, most people—and this includes the doctors and psychiatrists—have never taken a course on gender studies or even critically engaged with the concept of gender. If I think back to my teenage years, I would have felt a lot better about myself if there had been a space where I could safely discuss my gender identity, with the reassurance that no matter what, I was a valid human being. Gender clinics did not provide this space then, and I’m not convinced that they do today.
While we’ve come a long way, conservatives and so-called radical feminists are getting more and more confident about questioning the fundamental rights of people of trans experience. Their superficial appeals to science and hand-wringing about women’s safety in hypothetical scenarios betray a visceral disgust of the other. This is obvious when it comes to conservatives, but subtler when it comes to reactionary feminists, slipping through only when they talk about whom they deem to be acceptable women. Some, such as Germaine Greer, are quite open about this:
Nowadays we are all likely to meet people who think they are women, have women’s names, and feminine clothes and lots of eyeshadow, who seem to us to be some kind of ghastly parody, though it isn’t polite to say so.
The fundamental argument here is that some women are allowed to wear makeup and feminine clothes, while others—determined by Greer’s subjective experience—should know their role and conform to Greer’s arbitrary standards. Although feminist critiques of dress can be insightful, it’s a strange kind of feminism that seeks to divide women into categories and police their gender expression.
The logical conclusion of this rhetoric is J.K. Rowling, one of the most privileged women in the world, weaponizing her grief over her own sexual assault to put my fundamental rights up for debate. Having seen my male privilege evaporate 15 years ago, and having been on the receiving end of the degrading treatment women around the world have come to expect, I understand her grief. I’d march with her if she were discriminated against on the basis of being a woman. But would she march with me?




